Question 01
Which sites create downstream safety, quality, and data-cleaning burden after adjusting for patient acuity?
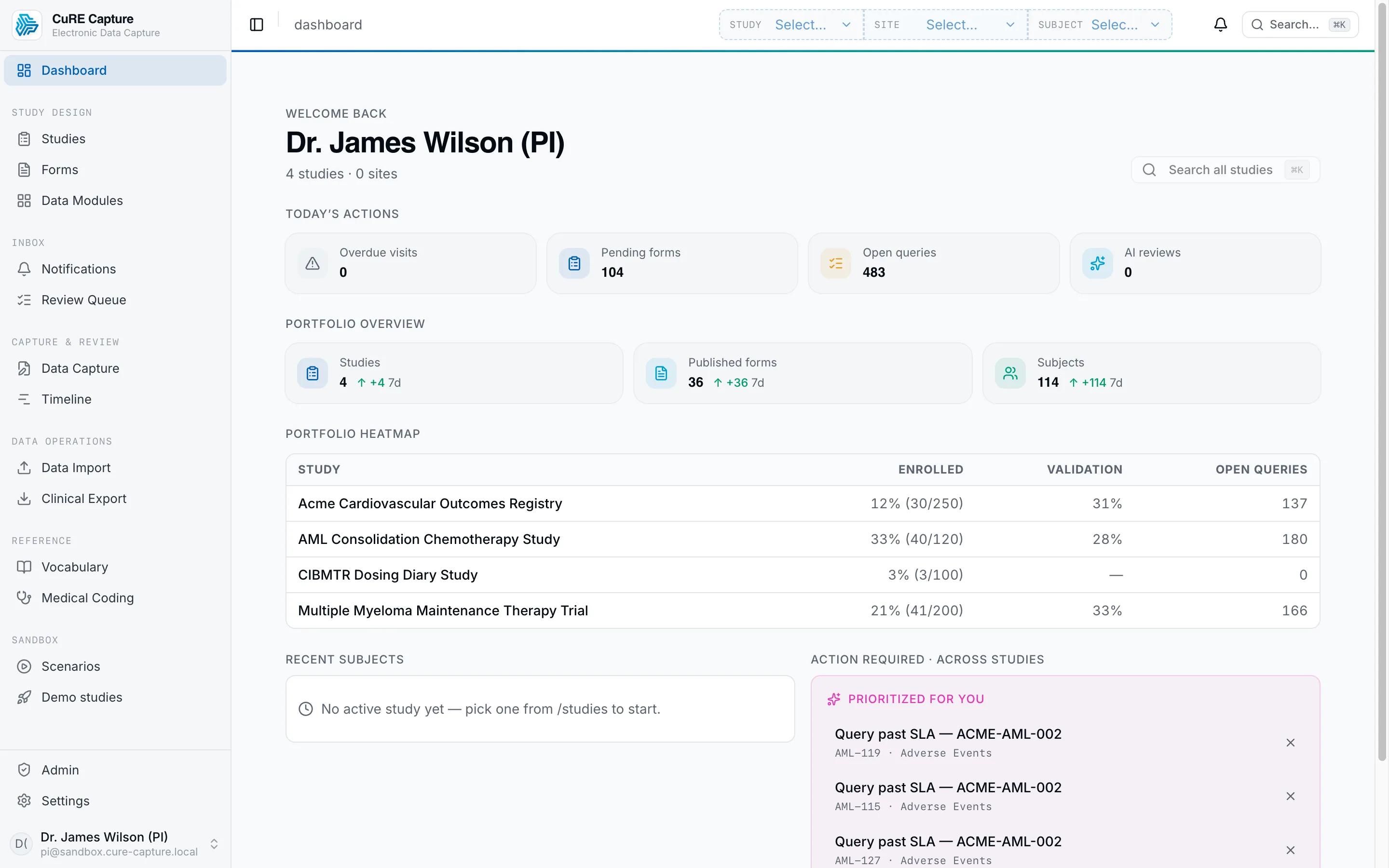
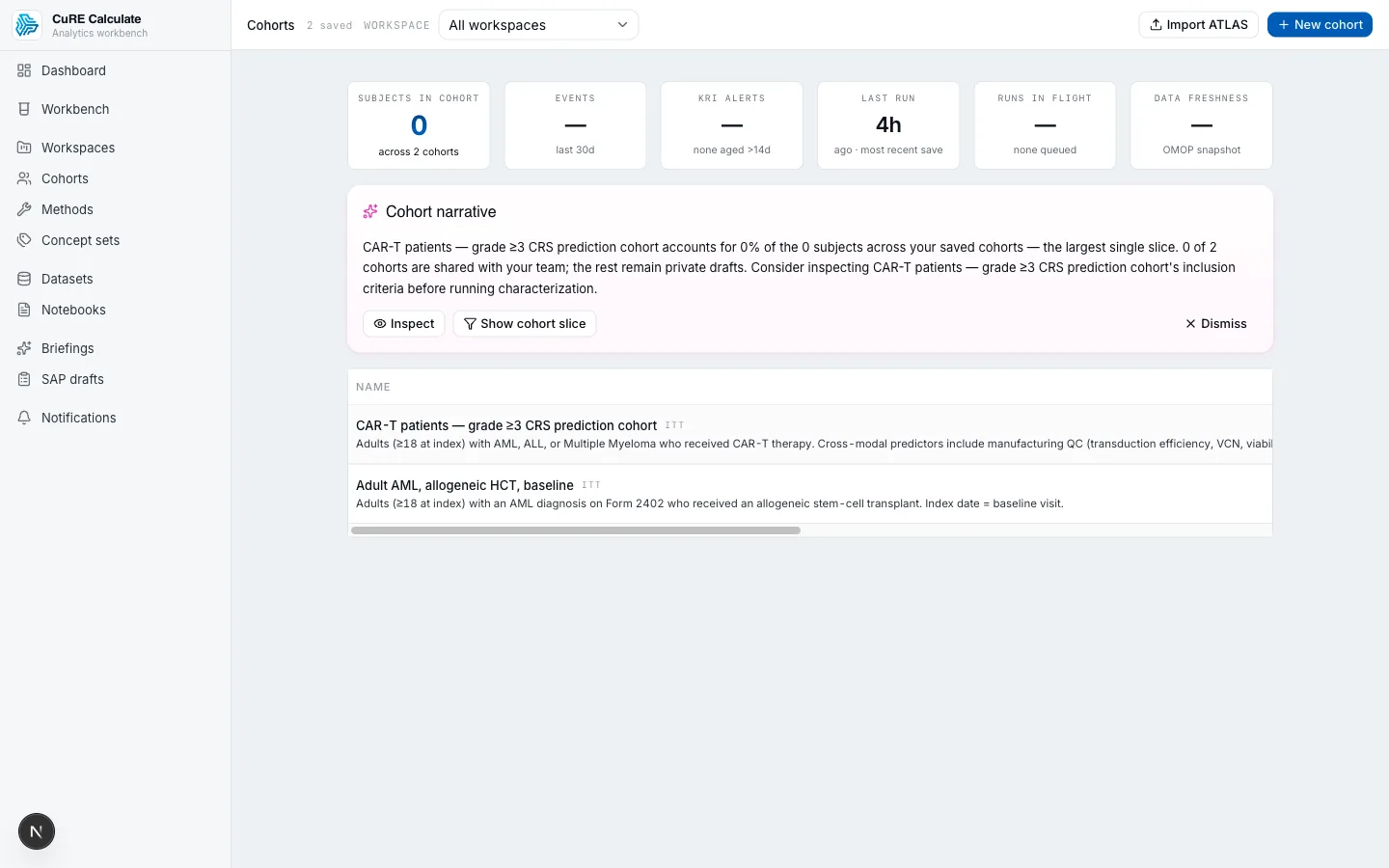
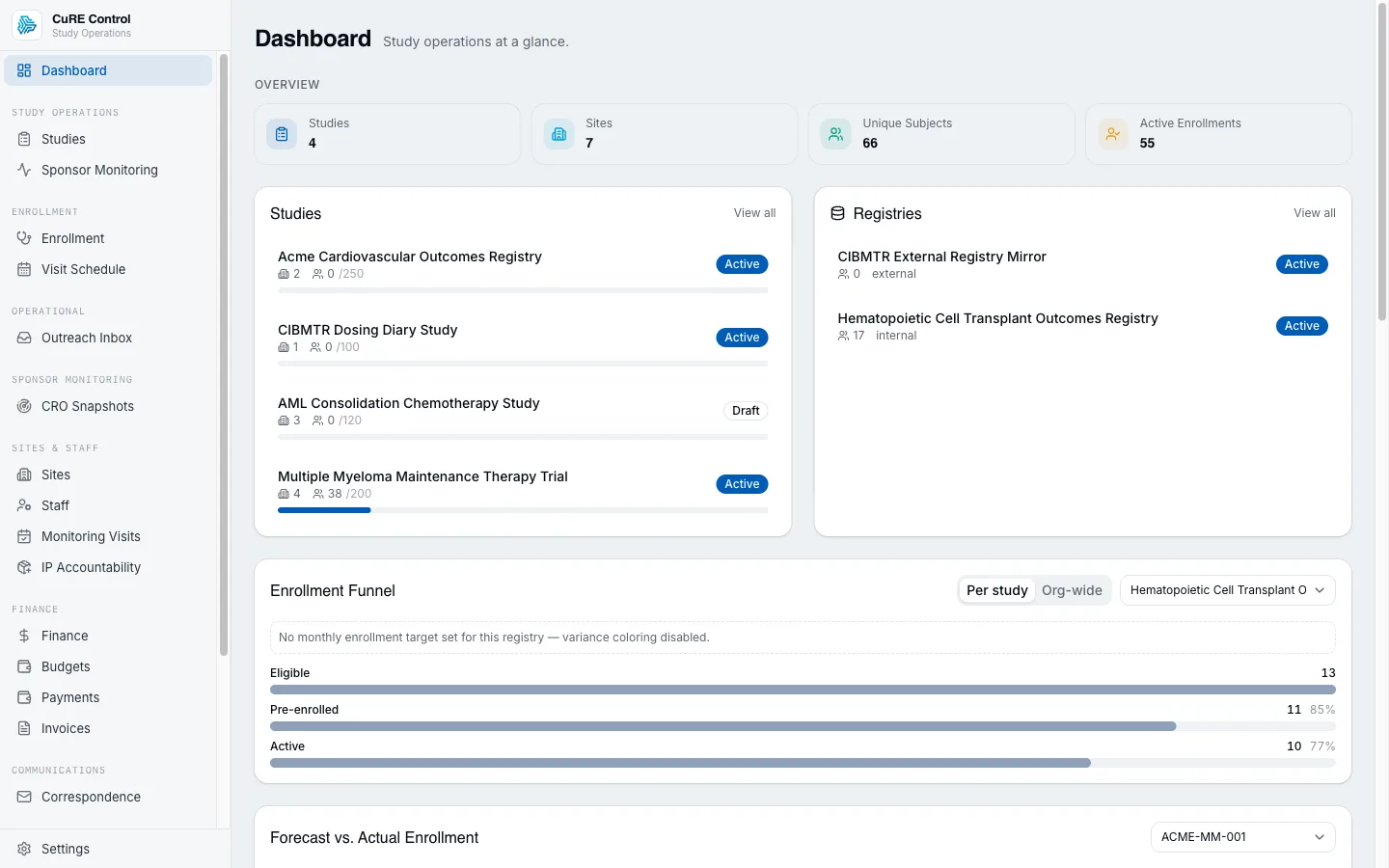
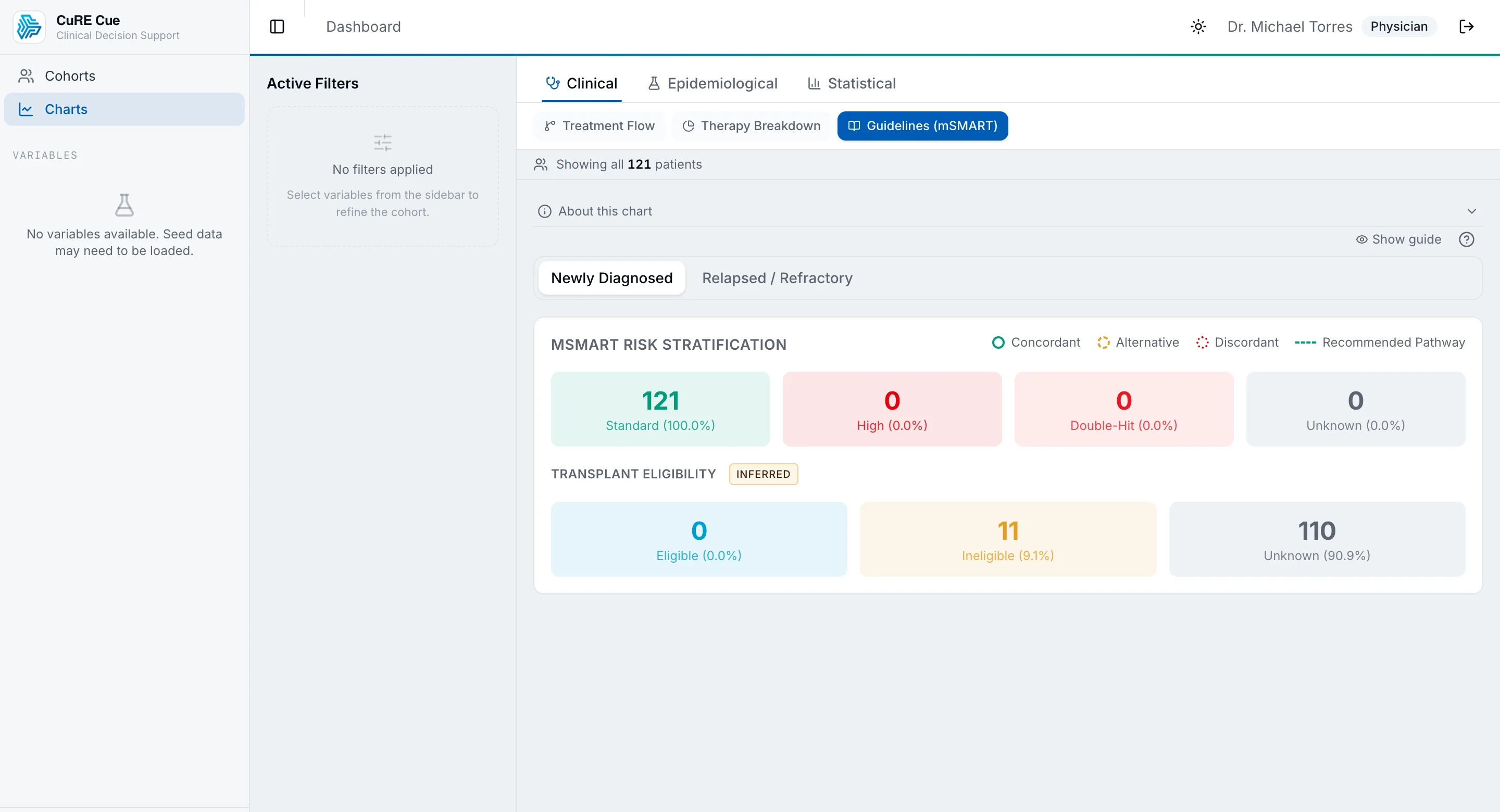
EDC, operations, safety, RBQM, EHR, and outcomes resolve to one governed record.
Site quality is measured by total evidence burden, not just enrollment speed.