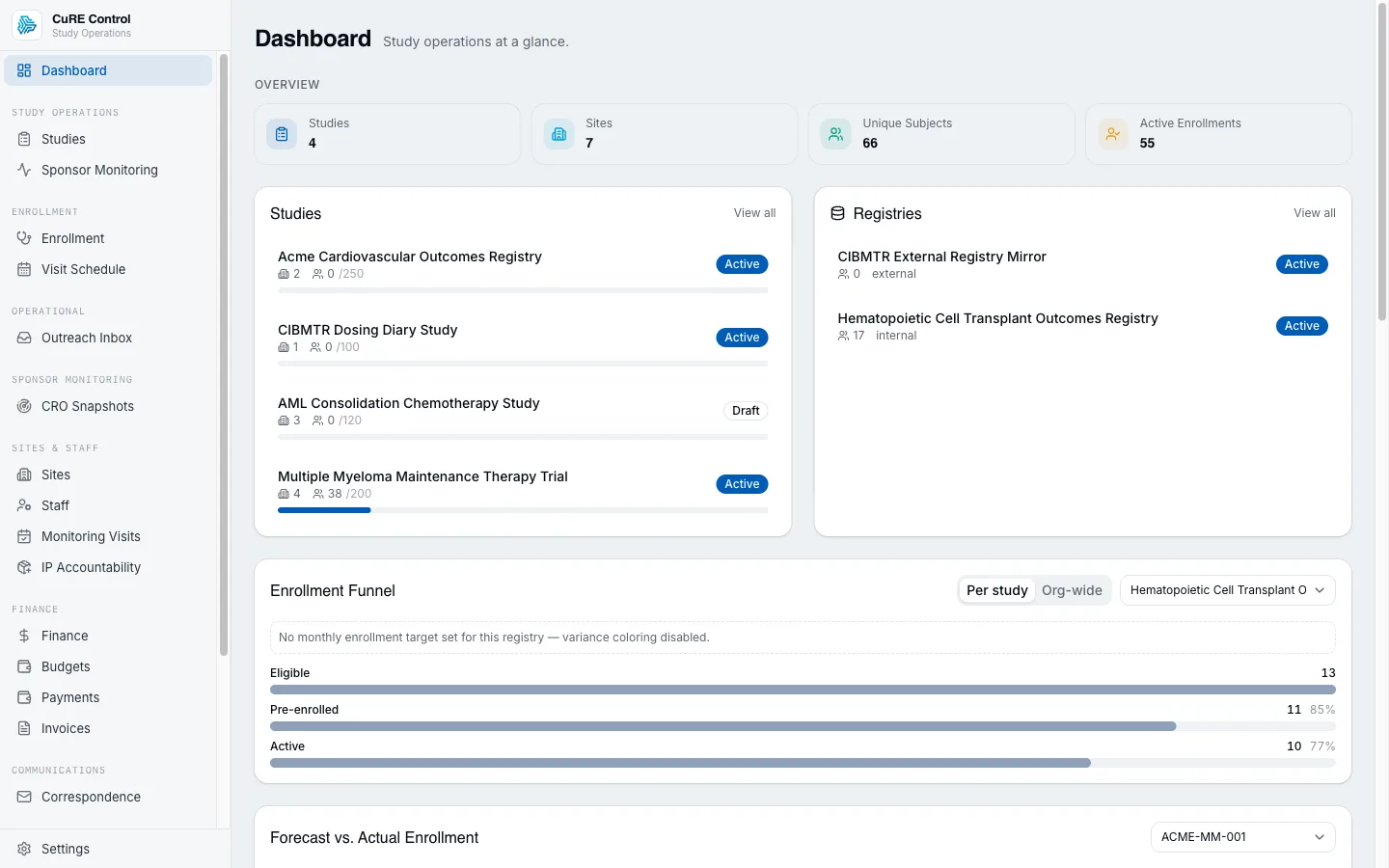
CTRMS · Study & registry operators
CuRE Control
RWD-native study operations and registry lifecycle, with a persona-aware tenant model.
What it does
RWD-native study operations and registry lifecycle, with a persona-aware tenant model. Patient → Data → Studies: registries and trials layer on longitudinal patient data instead of trapping each patient record inside one protocol.
Key capabilities
- Study setup + enrollment
- Registry lifecycle (enrollment → submission)
- Data-flow consent gates + re-consent tracking (governance)
- Tenant + identity management (CRO orgs and sponsors as first-class types)
- Canonical USDM-shaped study-design model (the MDR design plane)
- Orchestration of Conduct + downstream products
- Design-time Trial-Design Explorer (operating characteristics, GSD sizing, allocation-rule evaluation — consumes Calculate)
- Risk-based monitoring visit planning (Caliber KRI-driven)
- CTA / site-contract lifecycle
- Research billing / coverage analysis
- Cost accrual & budget-vs-actual
- RWD-conditioned feasibility & site selection
What sets it apart
- Patient → Data → Studies: registries and trials layer on longitudinal patient data instead of trapping each patient record inside one protocol.
- Anchors the canonical, USDM-shaped study-design model — the Metadata Repository spine that the CRFs, SDTM mapping, and define.xml downstream are generated from, not hand-rebuilt against.
- Clinical-ops parity is named directly: startup, site activation, monitoring trips, milestones, issues, and enrollment funnels belong in Control.
- The RBQM loop closes inside the platform: a Caliber KRI/QTL breach re-triggers and re-scopes monitoring visits — the ICH E6(R3) RFP bar.
- CRO CSV → OMOP → live Control views: outsourced study data can become governed operational signal without rebuilding the study stack.
- Owns the canonical user/org graph — every other app resolves identity through Control.
- Eligibility surfaced at the point of care in Cue warm-hand-offs into Control's enrollment funnel — the referral-to-enrollment gap most CTMSs leave open.
- As the Translational bundle extends upstream toward first-in-human IND, Control orchestrates the IND journey — preclinical-to-FIH milestones on the same governed record.
Walk a study through startup, then watch its enrollment funnel
A CTMS stands a study up — protocol, contract, IRB, per-site activation — and then watches subjects flow through the enrollment funnel. Switch the study phase and the stage matrix reshapes; pick a site and drag its screening and enrollment counts, and watch the cumulative funnel, the screen-fail rate, and the recruitment-health band recompute — graded against each site's slice of the planned-enrollment curve. The all-sites panel scores every synthetic site the same way.
A synthetic study — ravucizumab (VELT-042), 240-subject target across 4 sites.
Funnel stages: Screened → Enrolled → Randomized → On Treatment → Completed
Activated — open to screening, so it contributes to the funnel.
These are the mutually-exclusive current-status counts. The funnel shows the cumulative "ever reached" count — every later stage rolls up into the earlier bars.
Study-startup milestones
Recruitment health grades this site's enrolment against its slice of the planned-enrollment trapezoid — below 75% of plan is lagging, above 110% is leading. With no site target it falls back to the site's conversion vs. the study-wide rate.
All sites · recruitment health
| Site | Screened | Enrolled | Conv. | Health |
|---|---|---|---|---|
| Northwood Medical Center · Site 104 | 50 | 42 | 84% | Leadingtarget |
| Cedar Valley Research · Site 211 | 39 | 29 | 74% | On tracktarget |
| Harborview Clinical · Site 278 | 26 | 12 | 46% | Laggingtarget |
| Summit Trials Institute · Site 340IRB approved | 0 | 0 | — | No activitytarget |
Every count and band is computed in your browser from the synthetic status snapshots — no backend. Notice the funnel is cumulative: a site with a low current Screened count can still show a tall Screened bar because everyone downstream passed through it. And a busy site with a high screen-fail rate isn't the same as a healthy one — recruitment health grades enrolment against the plan curve, not raw volume.
Why this is more than a toy
The funnel model and every recruitment metric are a faithful, dependency-free port of Control's real methodology, from three source files under apps/control/src/server/dashboard/: the funnel.ts enrollment-funnel stage model — the ADR-CTL-010 StudyType stage matrix (Phase III shows Randomized; long-term follow-up and observational studies relabel On Treatment → In Follow-up), the cumulative "ever reached stage X" derivation over mutually-exclusive snapshot statuses, and the terminal-status attrition annotations — the site-funnel.ts per-site comparison layer (screen→enroll conversion, screen-fail rate, enrolled share, and the recruitment-health band with its 0.75 lagging / 1.1 leading thresholds), and the plan.ts planned-enrollment curve — a piecewise-linear ramp/steady/taper trapezoid whose area equals the target — ported line-for-line. The startup-milestone chain makes the feasibility → screening activation handoff (ADR-CTL-066) legible: a site that hasn't been activated contributes nothing to the funnel, no matter how promising its feasibility count. Per ADR-PLT-044 all of this is Control's own operational read-math — pure, bound to no statistical-methodology artifact — so it lives in-app rather than in Calculate. Here it all runs entirely client-side on a synthetic study — no backend, no real data.
See CuRE Control in action
Every research ecosystem is unique. Let's discuss how CuRE can be configured for your needs.